

You may notice your gums bleed when you brush, feel tender, or have pulled away from your teeth. These are warning signs of periodontal disease, a group of infections that attack the tissue and bone that hold your teeth in place.
According to published research in BMC Oral Health (Haque et al., 2022), periodontal disease is one of the most common chronic inflammatory diseases in humans, affecting up to 90% of the global population.
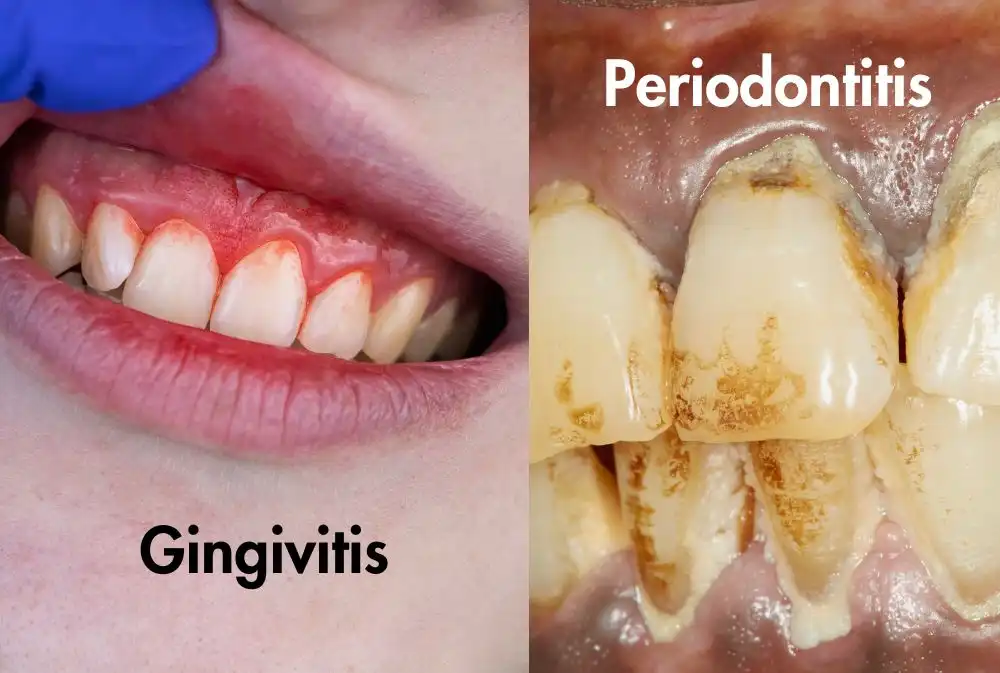
In its early stage, called gingivitis (inflammation of the gums), the bone and ligaments around your teeth are not yet damaged, and the condition can be reversed with better hygiene and professional cleaning.
But when it progresses to periodontitis (full-blown gum disease), the story changes. The infection creates deep pockets around your teeth; dark, warm, and moist spaces where harmful bacteria thrive.
Over time, these bacteria destroy the alveolar bone (the jawbone that holds your teeth in their sockets) and the periodontal ligaments (the tiny fibers that anchor each tooth). Once that bone is gone, it cannot simply grow back.
The disease can be classified in four stages, Stage I through Stage IV, where Stage IV represents the most complex and destructive level of bone and tissue damage.
In this article, we explore the latest scientifically backed treatment options for gum disease and explain how to choose the right trusted dental clinic in Dubai for effective long-term care.
- Key Takeaways
- From "Kill All Bacteria" to "Restore Balance": How Modern Dentistry Thinks Differently
- The 4 Golden Keys to Advanced Gum Disease Treatment
- Key #1: Local Drug Delivery Systems, Sending Medicine Exactly Where It's Needed
- Key #2: Modern Physical Therapies: Lasers, Light, and Sound Waves
- Key #3: Microbiome Therapy: Supporting the Mouth’s Natural Bacterial Balance Instead of Disrupting It
- Key #4: Host Immune Modulation and Stem Cell Therapy: Training Your Immune System to Stop Attacking Itself
- The Legend Table: Comparing the 4 Advanced Gum Treatments at a Glance
- Seeking World-Class Medical Care in Dubai? 🏥
- Why Does Advanced Treatment Cost More and Why It's Worth It
- What Happens If You Delay Treatment?
- How to Choose the Right Gum Disease Specialist
- Meet the Dental Team That Checks Every Box: King's College Hospital London, Dubai
- Gum Disease Treatment: Myths vs. Reality
- Summary
- FAQs
Key Takeaways
- Gum disease affects up to 90% of people worldwide, and standard antibiotics alone are increasingly failing due to antibiotic resistance.
- Bacteria inside dental plaque form “biofilms” fortress-like layers that can be 1,000× more resistant to antibiotics than free-floating bacteria.
- Modern dentistry has shifted its goal: instead of blindly wiping out all bacteria, the aim is now to restore a healthy balance in your mouth’s ecosystem.
- Four advanced approaches offer real results: (1) targeted local drug delivery, (2) laser and ultrasound therapies, (3) probiotic/microbiome therapy, and (4) host immune modulation with stem cells.
- Waiting too long to seek treatment can allow a manageable condition to progress into irreversible bone and tooth loss.

From “Kill All Bacteria” to “Restore Balance”: How Modern Dentistry Thinks Differently
For decades, the standard response to gum disease was to scrape off plaque, prescribe broad-spectrum antibiotics (medicines that kill many types of bacteria at once), and hope for the best. However, this method comes with a major limitation.
Recent periodontal research shows a major shift in treatment goals, moving away from simply eliminating bacteria and focusing instead on rebuilding balance within the oral microbiome. The reason for this shift? Traditional methods are starting to fail in ways that cannot be ignored.
Why Scaling and Standard Antibiotics Sometimes Fall Short
Understanding why traditional treatments have limitations helps you appreciate why more advanced options now exist.
1. The Biofilm Problem: Bacteria That Build Fortresses
The bacteria responsible for gum disease don’t just float around on their own. They organize into biofilms; complex, sticky communities that coat tooth surfaces and dive deep into gum pockets. Think of a biofilm like a thick gel made of bacterial cells, sugars, and proteins.
This structure is not just gross, it’s biologically hostile to treatment. The Haque et al. paper explains that bacteria inside a biofilm can be 1,000 times more resistant to antibiotics than the same bacteria swimming freely.
The biofilm’s outer layer blocks antibiotics from penetrating, and the bacteria inside grow more slowly and activate resistance genes.
Biofilms also act as a “resistance-sharing network.” Studies cited in the paper show that bacteria inside biofilms exchange antibiotic-resistance genes with each other at an accelerated rate, meaning the whole community gets tougher the more you attack it.
2. The Antibiotic Resistance Crisis: Medicines That No Longer Work
Antibiotic resistance, where bacteria evolve to survive drugs that once killed them, is a growing global crisis, and it’s happening inside mouths too.
- Some species of Porphyromonas gingivalis (one of the main culprits in gum disease) produce an enzyme called β-lactamase that destroys amoxicillin before it can work. In one study, this resistance enzyme was detected in 64% of patients with periodontal disease.
- 21.6% of P. gingivalis isolates from periodontitis patients were resistant to metronidazole, a common first-line antibiotic.
- Resistance to tetracycline, erythromycin, and clindamycin has also been reported among multiple gum disease bacteria.
This means that prescribing the same old antibiotics may do more harm than good: they disrupt your entire oral ecosystem without reliably eliminating the target bacteria.
3. Drug Side Effects: The Cost of Systemic Antibiotics
Systemic antibiotics (pills you swallow that travel through your entire bloodstream) affect the whole body, not just your gums. Clinical trials summarized in the paper recorded side effects including:
- Nausea and vomiting
- Diarrhea
- Stomach burning
- Candidiasis (a fungal infection, because antibiotics kill your protective bacteria too)
These aren’t rare exceptions, they are reported in multiple randomized controlled trials across different antibiotic regimens for gum disease.
The 4 Golden Keys to Advanced Gum Disease Treatment
Given the limitations above, researchers have been developing targeted, smarter approaches. Here are the four most evidence-supported categories, drawn directly from the 2022 BMC Oral Health review.
Key #1: Local Drug Delivery Systems, Sending Medicine Exactly Where It’s Needed
What is it?
Instead of swallowing an antibiotic pill that floods your bloodstream, a local drug delivery system places medicine directly inside the diseased gum pocket; in tiny, precisely engineered particles or gels.
How does it work?
The paper describes a range of delivery “vehicles” tested in clinical and pre-clinical studies:
- Nanofibers (ultra-thin threads made from materials like polycaprolactone, or PCL): Metronidazole or doxycycline loaded into nanofibers showed clinically significant improvements in plaque index (how much plaque is on the teeth), pocket depth (how deep the gum pockets are), and gingival index (how inflamed the gums are).
- Liposomes (tiny fat-based bubbles that encapsulate drug): Minocycline delivered this way showed biocompatibility and improved the conditions of rat periodontitis in studies. A minocycline nanoliposome formulation strongly inhibited a key inflammatory signal for up to 60 hours.
- Polymersomes (synthetic bubble-like particles): When antibiotics were enclosed in polymersomes, they significantly decreased the number of P. gingivalis bacteria in infected cell models.
- Chitosan nanoparticles (chitosan is a natural material derived from shellfish): Doxycycline loaded into these showed 75% drug entrapment efficiency and demonstrated antimicrobial activity against P. gingivalis.
- Microspheres (tiny beads): Minocycline microspheres placed in pockets resulted in reduced pocket depth at 6 months and significantly less bleeding on probing (a key clinical measure of gum inflammation).
Why it matters
By delivering the drug locally and slowly releasing it over time, this approach achieves higher drug concentrations exactly where they’re needed, while dramatically reducing the exposure (and side effects) to the rest of your body.
Key #2: Modern Physical Therapies: Lasers, Light, and Sound Waves
What is it?
A group of non-antibiotic treatment methods that use light energy or sound waves to fight infection and reduce inflammation.
Methylene Blue-Mediated Photodynamic Therapy (MBPDT)
Photodynamic therapy = using a light-activated dye to kill bacteria or reduce inflammation
In MBPDT, a dye (methylene blue) is applied to the gum area and then activated with a specific wavelength of light. The research paper notes that MBPDT triggered apoptosis (programmed cell death; a clean, controlled process) in inflamed macrophages (immune cells that drive tissue destruction) via oxidative stress pathways. It also led to lower levels of two key inflammatory proteins (IL-1β and TNF-α) that are responsible for much of the bone and tissue damage in periodontitis.
Laser-Based Photothermal Therapy (PTT) with Indocyanine Green (ICG)
Photothermal = using heat generated by light to treat tissue
ICG (indocyanine green) is a dye that, when activated by a diode laser, generates precise heat to destroy bacteria and reduce inflammation in a targeted area. Clinical data cited in the paper showed a reduction of IL-1β and MMP-8 (an enzyme that breaks down gum tissue) at 6 months post-treatment in patients with gingival (gum) inflammation.
Low-Intensity Pulsed Ultrasound (LIPUS)
Ultrasound = sound waves beyond human hearing that can stimulate tissue at the cellular level
LIPUS delivers gentle, pulsed sound waves to periodontal tissues. According to the paper, treatment with LIPUS suppressed a range of inflammatory cytokines (signaling proteins that cause inflammation), including IL-1a, IL-1b, IL-6, and IL-8; at the transcription level (i.e., it reduced their production at the source). It was also shown to reduce the levels of TNF-α produced by periodontal ligament fibroblasts (connective tissue cells in the gum).
Guided Biofilm Therapy (GBT) with Erythritol Air-Polishing
A randomized controlled trial cited in the paper found that guided biofilm therapy combined with erythritol (a sugar alcohol) powder and ultrasonic piezo instruments is effective at disrupting biofilms in periodontal disease, without antibiotics.
Key #3: Microbiome Therapy: Supporting the Mouth’s Natural Bacterial Balance Instead of Disrupting It
What is it?
Rather than wiping out all bacteria (good and bad alike), microbiome therapy focuses on reintroducing or reinforcing the beneficial bacteria that naturally keep the mouth healthy.
Probiotic Therapy
Probiotics are beneficial live bacteria you introduce to compete with and suppress harmful ones. The paper reviews recent clinical trials showing that probiotic administration improves bacterial dysbiosis (an imbalanced, disease-promoting bacterial community) in periodontal patients.
Key findings from the paper:
- Lactobacillus reuteri proved as effective as conventional interventions in reducing dental biofilm-induced problems.
- A study of 51 patients showed that yogurt supplemented with Bifidobacterium animalis significantly improved inflammatory markers of gum tissue and reduced bacterial plaque.
- Isolates including Lactobacillus salivarius, L. plantarum, L. rhamnosus, and L. paracasei showed the strongest antimicrobial properties, confirmed by international probiotic evaluation guidelines.
Beneficial bacteria help protect the mouth by creating a natural defense system that limits the growth and spread of harmful pathogens like P. gingivalis.
Oral Microbiota Transplant (OMT) Therapy
This is the frontier edge of periodontal science. Inspired by fecal microbiota transplants (which have successfully treated infections like Clostridium difficile and Crohn’s disease), oral microbiota transplant therapy involves transferring the microbiome from a healthy donor’s mouth to a patient with periodontitis.
The paper notes that protocols for OMT have already been proposed, and a recent study protocol demonstrated that this approach could effectively treat periodontal disease by modulating the oral microbiota. For this to work, a thorough medical history and microbiota analysis of the donor is essential.
Key #4: Host Immune Modulation and Stem Cell Therapy: Training Your Immune System to Stop Attacking Itself
What is it?
In periodontitis, it’s not just the bacteria that destroy your bone, it’s also your own immune system, which sometimes overreacts and causes more damage than it prevents. Host modulation therapy aims to correct this overreaction.
Immunomodulatory Drug Therapy
Several natural and pharmaceutical compounds have been studied:
- Resveratrol (a compound found in red grapes): Inhibits a key inflammatory signal (NF-kB) in macrophages and shows immunomodulatory effects against F. nucleatum.
- Metformin (a diabetes drug): Reduces inflammatory markers and has shown promise in periodontal patients with diabetes.
- Curcumin (the active compound in turmeric): Reduces phagocytic activity in inflamed macrophages, with anti-inflammatory properties documented against periodontal disease.
- Sub-antimicrobial dose doxycycline (a very low dose of antibiotic, too low to kill bacteria, but enough to reduce inflammation): Inhibits MMP-8 (an enzyme that destroys gum tissue), reduces inflammatory markers in gingival crevicular fluid, and has been shown in multiple studies to reduce pocket depth and improve clinical attachment level.
Stem Cell Therapy
This is the most cutting-edge direction in gum disease research. Different types of stem cells (master cells that can develop into many types of tissue) have been investigated:
- Periodontal Ligament Stem Cells (PDLSCs): Can convert destructive immune cells (M1 macrophages) into healing ones (M2 macrophages), suppress overactive B-cells, and enhance tissue regeneration.
- Gingiva-Derived Mesenchymal Stem Cells (GMSCs): Promote the switch from destructive to healing macrophage types, reduce inflammatory infiltration by neutrophils, and decrease pro-inflammatory cytokines like TNF-α and IL-1β.
- Dental Pulp Stem Cells (DPSCs): Decrease levels of TNF-α, IFN-γ, and IL-17; can regenerate different tissues including bone; and are easy to store.
The paper concludes that these stem cell approaches are “getting much attention for treating periodontal diseases.”
The Legend Table: Comparing the 4 Advanced Gum Treatments at a Glance
| Criteria | Local Drug Delivery | Laser / Ultrasound / PDT | Probiotics & Microbiome Therapy | Host Modulation & Stem Cells |
| Pain Level | Minimal, medicine is placed gently in the pocket | Generally low to moderate (laser may cause mild warmth) | None, oral probiotics or transplant | Low for drug therapy; moderate for stem cell procedures |
| Treatment Effectiveness | High for reducing pocket depth and bacterial load | High for reducing inflammation and biofilm; supports tissue regeneration | Moderate, best as adjunct; promising for prevention | High for controlling bone loss; stem cells show strong regenerative potential |
| Speed of Results | Improvements seen within weeks to 6 months | Cytokine and clinical improvements at 3–6 months | Gradual (weeks to months of consistent probiotic use) | Drug therapy: weeks; stem cells: months |
| Best Suited For | Patients with moderate-to-severe periodontitis (Stage II–IV); those who cannot tolerate systemic antibiotics | Patients with persistent inflammation; those seeking antibiotic-free options; smokers (evidence for laser adjuncts in smokers) | Patients in early-to-moderate stages; patients wanting to maintain healthy microbiome after treatment | Patients with severe bone loss; diabetic patients; Stage III–IV periodontitis |
| Recovery Time | Minimal, local application means no systemic recovery needed | Minimal to short | None, probiotics are taken daily like a supplement | Drug therapy: no downtime; stem cell therapy: varies by procedure type |
Seeking World-Class Medical Care in Dubai? 🏥
Nova Voya helps international patients seamlessly navigate advanced healthcare in Dubai. We connect you with top-tier medical specialists and accredited hospitals tailored precisely to your unique healthcare needs, ensuring a smooth, safe, and stress-free medical journey.
- ✔ Personalized matching with leading medical experts and premier facilities
- ✔ Full support with medical coordination, second opinions, and logistics
- ✔ Independent, honest guidance focused entirely on your health goals
*Medical tourism guidance, not clinical advice
Why Does Advanced Treatment Cost More and Why It’s Worth It
It is true that nano-delivery systems, laser therapies, and stem cell approaches cost more upfront than a simple scaling and antibiotic prescription. But the paper’s clinical findings offer a compelling financial logic.
Consider the progression: gingivitis → Stage I periodontitis → Stage II → Stage III → Stage IV.
Each stage brings more bone loss, more pocket depth, and more complexity. A Stage III or IV patient may require:
- Multiple rounds of surgical periodontal procedures
- Bone grafting (surgical procedure to restore lost jawbone)
- Dental implants (to replace lost teeth)
By investing in targeted local delivery of antibiotics that actually reach the bacteria, or laser therapy that disrupts biofilms without triggering resistance, or probiotics that maintain a healthy microbiome after treatment, patients can interrupt this progression before it reaches the expensive surgical stage.
The Haque et al. paper notes that sub-antimicrobial dose doxycycline, for example, achieved significant reductions in pocket depth and improvements in clinical attachment across multiple studies, and at a dose so low it doesn’t cause systemic side effects.
That is a cost-effective, evidence-based adjunct that many patients never hear about.
What Happens If You Delay Treatment?
Short answer: the window for reversal closes.
Gingivitis is reversible. At this stage, the bone and ligaments are intact. Improved hygiene and professional scaling can bring the gums fully back to health.
Periodontitis is not fully reversible. Once the bone and periodontal ligaments are destroyed, the paper is clear: only management and prevention of further loss is possible without regenerative procedures. The clinical manifestations include:
- Deep periodontal pockets (the space between your gum and tooth deepens, harboring more bacteria)
- Loose teeth
- Potential tooth loss
- Increased systemic (whole-body) inflammation, which the paper links to ongoing immune dysregulation
The bacteria responsible, particularly Porphyromonas gingivalis, Tannerella forsythia, and Treponema denticola (known as the “red complex”) are capable of evading the immune system, producing enzymes that break down tissue, and sharing resistance genes with neighboring bacteria. They do not stop on their own.
How to Choose the Right Gum Disease Specialist
When looking for a dentist or periodontist to treat advanced gum disease, the following qualities matter:
Evidence-Based Practice
Look for a clinician who follows AAP (American Academy of Periodontology) or EFP (European Federation of Periodontology) guidelines and stages periodontitis properly (Stage I–IV) before deciding on treatment.
Knowledge of Advanced Therapeutic Options
A specialist worth trusting should be familiar with and able to discuss: local drug delivery, photodynamic therapy, and microbiome considerations. If the only option offered is “scaling + antibiotics,” it may be worth seeking a second opinion for moderate-to-severe cases.
Minimally Invasive First Approach
The paper is clear that surgical procedures should only follow when non-surgical options have been deemed insufficient. A good specialist tries the least invasive effective route first.
Full-Mouth Assessment
Periodontal disease is a whole-mouth condition. A thorough specialist will assess every area, not just the area where you feel pain.
Transparency About Risks and Side Effects
Any clinician recommending systemic antibiotics should discuss the risk of antibiotic resistance, gut disruption, and potential side effects, not just the benefits.
Commitment to Long-Term Maintenance
The microbiome-based view of periodontal disease means that long-term health depends on ongoing maintenance and monitoring, not just a one-time fix.
Meet the Dental Team That Checks Every Box: King’s College Hospital London, Dubai
King’s College Hospital London, Dubai is located in Dubai Hills and brings British-standard healthcare to the UAE, with British-trained doctors, modern techniques, and evidence-based procedures at its core.
The hospital offers a wide range of services, from 24/7 emergency care and cardiology to allied health services like physiotherapy and dietetics and maintains dedicated clinics in Dubai Marina and Dubai Jumeirah.
For gum disease specifically, two dentists stand out:
Dr. Reshma Samir Naik: General Dentist & Implantologist
Qualifications: BDS, MFDS (Royal College of Surgeons, Edinburgh), Diploma in Dental Implantology (Cambridge University)
Locations: Dubai Marina Clinic | Dubai Jumeirah Clinic
Dr. Naik brings over 24 years of clinical experience across India, the United Kingdom, and the UAE. She began her career in the Maxillofacial department at Royal Preston Hospital and St George’s University Hospital in London before specialising in implantology and general dentistry in Essex and Northeast London.
Her areas of special interest align directly with the advanced treatment approaches discussed in this article:
- Full mouth rehabilitation
- Dental implants, including bone grafts and sinus lifts
- Root canal treatment (single-session)
- Crown and bridge placements
- Smile design and aesthetic dentistry
For patients at Stage III or IV periodontitis who face potential tooth loss, Dr. Naik’s combined expertise in implantology and restorative dentistry means the full continuum of care, from treating the disease to rebuilding the smile, is available in one place.
Dr. Anushay Ghaffar Khan: Lead General Dentist
Qualifications: BDS (University of Liverpool, 2017), Certified in Invisalign, Mini Smile Makeover, Totally Composite
Memberships: British Dental Association (BDA) | General Dental Council (UK)
Locations: Dubai Marina Clinic | Dubai Jumeirah Clinic
Dr. Anushay Ghaffar Khan trained within the Health Education North West Deanery, one of the UK’s most respected dental training programmes and went on to work with award-winning private practices in London, gaining deep experience in high-quality cosmetic and restorative dentistry.
Her approach is rooted in minimally invasive, evidence-based care, exactly what the research on advanced periodontal treatments calls for. She is also particularly skilled with anxious patients and children, offering a calm, patient-centred experience that makes attending appointments less daunting.
Her certifications in the Mini Smile Makeover and Totally Composite techniques reflect a commitment to doing as little damage as necessary to healthy tooth structure, a philosophy that fits naturally with the microbiome-preservation approach to gum disease treatment discussed in this article.

Gum Disease Treatment: Myths vs. Reality
| Myth | Fact (The Reality) |
| Antibiotics are the ultimate “cure” for gum disease. | Antibiotics are only temporary aids and are becoming less effective due to resistance. |
| The goal of treatment is to kill all bacteria in the mouth. | The goal is to restore balance (homeostasis), not total elimination. |
| Standard scaling (cleaning) is enough to treat advanced cases. | Deep pockets and complex biofilms often require adjunctive (additional) therapies. |
| Once gum disease is treated, it’s gone forever. | It is a chronic condition that requires ongoing maintenanceand microbiome management. |
| Gum disease surgery is always painful and invasive. | Modern Physical Therapieshave made treatment minimally invasive. |
| Lost jawbone will grow back naturally once the gums are healthy. | Bone loss is permanent unless specific regenerative treatments are used. |
| Gum disease only affects your mouth, not your overall health. | Periodontitis is a systemic inflammatory disease linked to heart disease and diabetes. |
Summary
Gum disease is far more than a cosmetic concern. It is a complex, progressive infection driven by biofilms increasingly resistant to antibiotics, fuelled by an immune system that can inadvertently destroy the very bone it is trying to protect.
The good news is that science has moved well beyond the era of “scale and prescribe.” Modern periodontal care now includes targeted local drug delivery, laser and ultrasound therapies, microbiome restoration, probiotics, and immune-focused treatments designed to improve outcomes while preserving the mouth’s natural balance.
If you are looking for a dental team in Dubai that combines British training standards with modern, evidence-based approaches to gum care, King’s College Hospital London, Dubai offers exactly that.
With clinics in Dubai Marina and Dubai Jumeirah, the hospital provides comprehensive dental services, from routine check-ups and preventive care through to complex restorative work and full mouth rehabilitation, supported by allied health services including dietetics and physiotherapy.
Whether you are in the early stages of gum disease or dealing with more advanced bone loss, their team is equipped to meet you where you are.
Don’t wait for Stage IV. Acting early gives you access to more treatment possibilities and better long-term outcomes.
🇬🇧 Save Your Natural Teeth with British-Standard Gum Care
Don’t let advanced periodontitis lead to tooth loss. Get an evidence-based treatment plan at King’s College Hospital London, Dubai, using the latest non-surgical and minimally invasive techniques discussed in this research.
- ✓ Expert Periodontal Assessment by British-trained specialists
- ✓ Advanced Adjunctive Therapies: Targeted drug delivery & laser-assisted care
- ✓ Convenient Locations: Dubai Hills, Dubai Marina, and Jumeirah
Trusted Care at
King’s College Hospital Dubai
What do you think is the biggest reason people delay treating gum disease: not noticing the symptoms early enough, fear of dental treatment, or assuming bleeding gums are “normal”?
FAQs
Yes, research shows it affects up to 90% of the global population in some form. Many people have it without realising, because early stages are often painless.
Better brushing prevents gingivitis, but once periodontitis develops, bacteria hide in deep pockets a toothbrush can never reach. Professional treatment is the only way to stop the disease from progressing.
Clinical trials in the research paper describe these therapies as generally well tolerated, with mild warmth at most. Significant pain is not typical for photodynamic or photothermal approaches.
Beneficial bacteria introduced through probiotics compete for space and make it harder for harmful bacteria to establish themselves. Clinical trials showed probiotics improved bacterial balance and reduced inflammatory markers in gum tissue.
Some immunomodulatory drug approaches are already used in clinical practice as adjuncts to standard treatment. Full stem cell therapies for gum regeneration are still largely in research stages but showing strong results.
Gingivitis is reversible gum inflammation where the bone is not yet damaged. Periodontitis is the advanced stage where bone and ligament destruction has already occurred and cannot fully reverse on its own.
A dentist measures your pocket depth, checks bone levels on X-rays, and assesses tissue attachment loss, this allows them to stage the disease from I to IV using international guidelines.
Antibiotics still have a valid role in certain stages when used alongside scaling and root planing. The key, as the research shows, is using them smarter and more targeted, not as the sole answer.
Scientific Source: This article is based on peer-reviewed research by Md Mahamudul Haque, Katherine Yerex, Anastasia Kelekis-Cholakis, and Kangmin Duan, “Advances in Novel Therapeutic Approaches for Periodontal Diseases,” published in BMC Oral Health, 2022, Vol. 22, Article 492. DOI: https://doi.org/10.1186/s12903-022-02530-6

