

Most people assume breathing problems come from allergies, congestion, or a deviated septum. But for a significant number of patients, the real culprit is something far more structural, and far less talked about: nasal valve insufficiency (NVI).
NVI is a distinct anatomic condition where the narrowest part of your nasal airway physically collapses during inhalation. It’s not mucus and not inflammation. It is your nose’s architecture working against you, every single breath.
The good news? A multicenter clinical study tracking 79 patients found that surgical correction of NVI delivers dramatic, lasting results; with a 65% reduction in nasal obstruction severity within just three months of surgery. And critically, patients who combined aesthetic goals with their functional procedure did just as well as those who had purely functional surgery.
If you’ve been told “it’s just allergies” but nothing seems to work, keep reading. These five warning signs suggest your breathing problem may actually be structural and correctable.
- Key Takeaways: (TL;DR)
- What's Actually Happening Inside Your Nose
- The 5 Warning Signs That Point to Nasal Valve Insufficiency
- Your Nose "Sucks In" on One or Both Sides When You Breathe Deeply
- You Feel Pinching or Narrowing at the Tip or Middle of Your Nose
- The "Finger Push" Test Instantly Improves Your Breathing
- Dr. Alireza Mohebbi
- You Have a Narrow Angle at the Internal Valve, Confirmed or Suspected
- Medical Treatments, Including Decongestants, Steroids, and Strips, Have Never Truly Solved It
- Quick Reference: Signs, Tests, and What They Mean
- What Does Surgery Actually Involve?
- Can You Fix My Breathing AND Improve Your Nose's Appearance?"
- Who Performs This Surgery and Why Surgeon Selection Matters
- Myth vs. Reality: Functional Rhinoplasty For Nasal Valve Insufficiency
- Summary
- FAQs
Key Takeaways: (TL;DR)
- Nasal valve insufficiency (NVI) is a structural condition (not allergies, not inflammation) where the nasal airway physically collapses during inhalation, and medication cannot fix it.
- The Bernoulli principle is the underlying physics: air accelerating through the narrowest nasal zones creates pressure that pulls weak lateral walls inward with every breath.
- A simple self-test (the modified Cottle maneuver), pulling your cheek gently outward, can signal NVI at home before you ever see a surgeon.
- Functional rhinoplasty using spreader and alar-batten grafts reduced nasal obstruction severity by ~65% within three months, confirmed across 79 patients and 10 major U.S. centers.
- Adding cosmetic goals to functional rhinoplasty does not compromise breathing outcomes; both groups improved equally (51.4 vs. 46.6 NOSE scale points, P = .49).
- The surgical failure rate was only 7.6%, and just 2.5% of all patients remained dissatisfied, making this one of the most reliably effective functional procedures in facial surgery.
- Outcomes were consistent across 12 different surgeons and 10 different centers, meaning the technique itself (not individual surgical style) drives the result.
- If conservative treatments have repeatedly failed, the problem is structural. Structural problems require structural solutions.

Dr. Alireza Mohebbi
ENT & Facial Plastic Surgeon · 20+ Years Experience
What’s Actually Happening Inside Your Nose
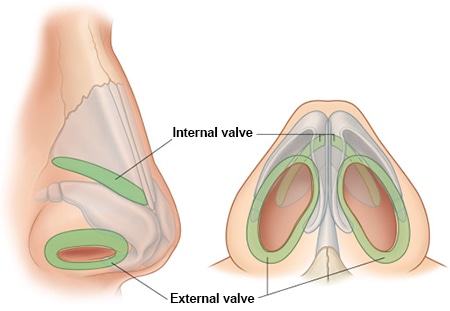
Your nasal airway has two key “checkpoints” where the passage narrows significantly:
The External Nasal Valve
This is the outermost gateway, formed by the alar rim on the outer side, the caudal septum and medial crus on the inner side, and the nasal sill at the base.
The Internal Nasal Valve
Located roughly 1.3–1.5 cm inside the nose, this is formed by the caudal edge of the upper lateral cartilage, the dorsal septum, and the head of the inferior turbinate. It’s the single narrowest cross-sectional area of the entire nasal cavity.
The Intervalve Area
Between these two valves lies the intervalve area, a zone entirely without cartilage support. Externally, it appears as the supra-alar crease, and in patients with structural weakness, this spot is particularly prone to collapse.
Here’s the physics that makes this dangerous:
as air rushes through these narrow zones, it accelerates and generates a drop in internal pressure. This is the Bernoulli principle, the same force that keeps a plane in the air, but in your nose, it works against you, pulling the soft lateral walls inward with every breath you take.
If those walls are structurally weak, they collapse. And no antihistamine fixes a structural problem.
The 5 Warning Signs That Point to Nasal Valve Insufficiency
The following signs are drawn directly from the clinical criteria used to diagnose NVI in the Yeung et al. 2016 multicenter study. They represent what 12 surgeons across 10 major U.S. centers looked for when evaluating patients.
Your Nose “Sucks In” on One or Both Sides When You Breathe Deeply
This is the hallmark of NVI. During a deeper-than-normal breath, you may notice the side wall of your nose (near the alar rim or mid-sidewall) visibly pulling inward. This lateral wall collapse is the primary physical manifestation of nasal valve weakness.
Unlike nasal congestion, which feels like pressure or fullness, valve collapse feels like sudden restriction, as though the airway clamps shut mid-breath. Athletes and people who exercise regularly often notice this first during exertion.
If breathing through your nose feels like breathing through a straw that kinks when you inhale harder, this is a red flag worth discussing with a surgeon.
You Feel Pinching or Narrowing at the Tip or Middle of Your Nose
The study’s diagnostic framework specifically identified supratip or middle-vault pinching as a clinical sign of NVI. This refers to an observable or palpable narrowing in the area just above the nasal tip or along the mid-portion of the nasal bridge.
In some patients, this pinching is visible externally, the nose appears narrow or pinched from the front. In others, it’s primarily a functional problem felt as airway resistance, even when the nose looks proportionate from the outside.
This sign is particularly relevant for patients who’ve had prior rhinoplasty. Post-surgical scarring and changes to cartilage support can create exactly this kind of structural narrowing, and a second functional procedure may be necessary to restore proper airflow.
The “Finger Push” Test Instantly Improves Your Breathing
This is one of the most practical self-tests a patient can perform, and it’s also the basis of a formal clinical tool called the Cottle or modified Cottle maneuver.
Here’s how it works:
place your fingertip gently on your cheek, just beside your nose, and pull the skin slightly outward. If your breathing immediately feels easier or more open, you’ve just simulated what structural support of the lateral nasal wall would do.
Surgeons in the 2016 study used this maneuver as a standardized assessment tool, rating the degree of improvement on a defined four-point scale. The majority of study participants showed moderate to substantial improvement with this test, confirming that their obstruction was structural, not mucosal.
If you notice this at home, it’s worth mentioning to a specialist. This simple test is highly meaningful diagnostically.
Dr. Alireza Mohebbi
ENT & Facial Plastic Surgeon · 20+ Years Experience
You Have a Narrow Angle at the Internal Valve, Confirmed or Suspected
The internal nasal valve angle (the angle between the upper lateral cartilage and the dorsal septum) normally measures around 10–15 degrees. When this angle is too narrow, either congenitally or following cosmetic rhinoplasty, even normal breathing produces significant resistance.
This is something a qualified surgeon assesses during a clinical nasal examination. Patients often describe the sensation as a deep, invisible restriction, as though the blockage is “inside” the nose rather than at the tip. It’s frequently misdiagnosed as a septal deviation, which leads to septoplasty procedures that don’t fully resolve the problem.
Medical Treatments, Including Decongestants, Steroids, and Strips, Have Never Truly Solved It
This is perhaps the most important sign of all: failed conservative management.
All patients enrolled in the 2016 study had experienced no meaningful improvement with medical or conservative treatment. This is a defining criterion for surgical candidacy, not because surgery is a last resort, but because it confirms the obstruction is structural rather than inflammatory.
If you’ve tried nasal sprays, antihistamines, nasal strips, and even breathing exercises, and still wake up congested, mouth-breathe through the night, or feel unable to draw a full breath through your nose; your problem likely isn’t responding because it can’t. Structure doesn’t respond to medication.
This is precisely the patient profile that functional rhinoplasty is designed for.
Quick Reference: Signs, Tests, and What They Mean
| Warning Sign | What It Looks/Feels Like | Clinical Term |
| Nose collapses inward when breathing | Visible or felt lateral wall collapse during inspiration | Lateral wall / alar rim collapse |
| Pinching at tip or mid-nose | Narrow appearance or sensation of restriction above the tip | Supratip or middle-vault pinching |
| Finger pull improves breathing instantly | Pressing cheek outward opens the airway noticeably | Positive Cottle / modified Cottle maneuver |
| Deep internal restriction, not at tip | Feeling of blockage deep inside, hard to localize | Narrow internal nasal valve angle |
| No improvement from medication or nasal strips | Treatments address inflammation, not structure | Failed conservative management |
What Does Surgery Actually Involve?
Functional rhinoplasty for NVI centers on cartilage reconstruction; specifically, the use of two types of grafts that the 2016 study identified as the most widely accepted and reliable method for treating this condition.
The Spreader Graft
Placed along the dorsal septum and extending the length of the upper lateral cartilage (typically 15–30 mm, with extended versions exceeding 30 mm), the spreader graft widens the internal nasal valve.
It essentially “props open” the angle that collapses under inspiratory pressure. In the study, 77% of all patients received a spreader graft, with higher usage in the aesthetic-functional group, largely because hump reduction procedures are often performed alongside.
The Alar-Batten Graft
This graft targets the area of maximum collapse or pinching along the lateral nasal wall. It’s positioned to support the external valve zone and the intervalve region, that cartilage-free area that’s most vulnerable to dynamic collapse. Placement is customized based on where each patient’s collapse occurs. In the study, 76% of patients received an alar-batten graft.
Cartilage material is taken from the septum (used in 65% of cases), the ear (28%), or the rib (18%), depending on what’s available and the extent of reconstruction needed.
Can You Fix My Breathing AND Improve Your Nose’s Appearance?”
Yes, and the clinical evidence supports it.
This was one of the core questions the 2016 study set out to answer. Researchers compared two groups:
- 31 patients who underwent purely functional rhinoplasty (structural correction only)
- 48 patients who underwent aesthetic-functional rhinoplasty (structural correction + cosmetic goals, including tip refinement, hump reduction, or osteotomies)
The result?
No statistically significant difference in breathing outcomes between the two groups.
The functional group improved by an average of 51.4 points on the NOSE scale. The aesthetic-functional group improved by 46.6 points. The difference is clinically negligible.
Adding tip sutures, cephalic trim, projection changes, hump reduction, or even osteotomies to a functional procedure did not compromise breathing outcomes. Neither did it enhance them; the structural reconstruction carried the functional benefit independently.
This finding has significant real-world implications: patients no longer need to choose between breathing better and looking the way they want.
Who Performs This Surgery and Why Surgeon Selection Matters
The 2016 study enrolled surgeons from the American Academy of Facial Plastic and Reconstructive Surgery who performed at least three such procedures per month. Centers included institutions like Johns Hopkins, NYU Langone, University of California, San Francisco, University of Minnesota, and University of Virginia.
One finding worth highlighting: despite individual variations in technique, cartilage source, and graft dimensions across 12 surgeons and 10 centers, outcomes were statistically equivalent. Analysis of variance showed no significant difference in results between centers.
This points to something important: when performed by experienced, qualified surgeons using standardized surgical principles, spreader and alar graft reconstruction, functional rhinoplasty produces consistently strong outcomes regardless of which specific surgeon or center performs it.
That said, the diagnosis still requires expert clinical judgment. There is no single lab test or imaging tool that definitively diagnoses NVI. A skilled surgeon’s physical examination, including the Cottle maneuver and assessment of valve anatomy, remains the gold standard.
For patients considering this procedure, Roya Medical Center Dubai offers access to experienced rhinoplasty specialists who evaluate both the functional and aesthetic dimensions of nasal surgery using a structured clinical approach.
The only thing harder than struggling to breathe
is discovering functional rhinoplasty
could have fixed it beautifully.
Book Your Free Consultation
Myth vs. Reality: Functional Rhinoplasty For Nasal Valve Insufficiency
| Myth | Reality |
| “My breathing problems are just allergies.” | NVI is structural; antihistamines and sprays cannot fix a collapsing airway. |
| “If my nose looks fine, my breathing must be fine.” | Many NVI patients have no visible external deformity. The problem is internal architecture. |
| “Rhinoplasty is only cosmetic, it won’t help my breathing.” | Functional rhinoplasty is specifically designed to restore airflow, not change appearance. |
| “Adding cosmetic work will compromise my breathing results.” | “Rhinoplasty is only cosmetic; it won’t help my breathing.” |
| “Septoplasty already failed, so surgery won’t help me.” | Septoplasty targets the septum, not the valve. NVI requires a different procedure entirely. |
| “Functional rhinoplasty results depend entirely on which surgeon you choose.” | Outcomes were statistically equivalent across 12 surgeons and 10 centers when standardized techniques were used. |
| “If surgery doesn’t work, it means the diagnosis was right but the technique failed.” | Some failures reflect inaccurate initial diagnosis, not surgical error; proper pre-op evaluation is critical. |
| “I need to wait until symptoms are severe before considering surgery.” | Clinical evidence shows that combining aesthetic and functional goals produces equivalent breathing outcomes. |
Summary
For decades, the conversation around rhinoplasty has been dominated by aesthetics. But the clinical evidence is clear: the nose is first and foremost a functional organ. For patients with nasal valve insufficiency, where the structure itself is the problem, cartilage graft reconstruction using spreader and alar grafts delivers measurable, lasting improvement in breathing quality.
What the 2016 multicenter study confirmed, across 79 patients and 10 centers, is that this improvement doesn’t require a trade-off. Patients who wanted both better breathing and a nose they felt confident about achieved both, with outcomes statistically identical to those who pursued functional correction alone.
If you recognize the five warning signs described above, especially if conservative treatments have repeatedly failed, a consultation with a surgeon experienced in functional rhinoplasty is the logical next step. The problem is structural. And structural problems have structural solutions.
Seeking World-Class Medical Care in Dubai? 🏥
Nova Voya helps international patients seamlessly navigate advanced healthcare in Dubai. We connect you with top-tier medical specialists and accredited hospitals tailored precisely to your unique healthcare needs, ensuring a smooth, safe, and stress-free medical journey.
- ✔ Personalized matching with leading medical experts and premier facilities
- ✔ Full support with medical coordination, second opinions, and logistics
- ✔ Independent, honest guidance focused entirely on your health goals
*Medical tourism guidance, not clinical advice
You’ve lived with the breathing difficulty this long, but what made you finally start looking for answers? Was it a specific moment, or just years of small frustrations adding up?
FAQs
Nasal valve insufficiency (NVI) is a structural condition where the narrowest part of the nasal airway physically collapses during inhalation, blocking airflow; not caused by mucus, allergies, or inflammation.
Pull your cheek gently outward beside your nose. If your breathing instantly improves, this is a positive modified Cottle maneuver, a key clinical sign of NVI.
Yes. A multicenter study of 79 patients found no significant difference in breathing outcomes between patients who had functional surgery alone and those who combined it with cosmetic goals.
Clinical research showed an average 65% reduction in nasal obstruction severity within three months of surgery, measured by the validated NOSE scale.
Results are stable over time. The 2016 multicenter study confirmed that breathing improvements at three months remained consistent at both six- and twelve-month follow-ups.
The two primary grafts are the spreader graft (widening the internal valve) and the alar-batten graft (supporting the collapsing lateral wall). Cartilage is taken from the septum, ear, or rib.
Not necessarily. NVI is caused by lateral wall weakness, not septal deviation. Septoplasty alone is insufficient for patients whose primary problem is valve collapse.
The Nasal Obstruction Symptom Evaluation (NOSE) scale is a validated, disease-specific quality-of-life tool that scores nasal obstruction severity from 0 (none) to 100 (maximum).
Scientific Source: This article is based on peer-reviewed research by Andrea Yeung, Basil Hassouneh, and David W. Kim, “Outcome of Nasal Valve Obstruction After Functional and Aesthetic-Functional Rhinoplasty”, published in JAMA Facial Plastic Surgery, 2016, Vol. 18(2), pp. 128–134. DOI: https://doi.org/10.1001/jamafacial.2015.1854

